
Your equipment failed during a critical procedure—here is why. Picture a complex orthopedic procedure on a 50-kilogram Mastiff. The surgeon relies on microscopic precision, but midway through the operation, the operating platform drifts downward by two inches. The sterile field shifts, the surgical site alignment is compromised, and the team must pause to manually recalibrate the elevation. This scenario is a common symptom of procurement failures where dynamic load limits and actuator specifications were misaligned with actual clinical demands.
For procurement managers and hospital directors, investing in clinical infrastructure requires looking beyond superficial aesthetics. The decision to integrate high-quality veterinary surgical tables impacts daily operational efficiency, staff ergonomics, and patient safety. A superficial understanding of lift mechanisms, material fatigue, and weight tolerances invariably leads to premature equipment failure, inflated maintenance budgets, and compromised clinical outcomes.
Why Your Last Purchase Underperformed: The Stability Crisis
In many high-volume veterinary practices, equipment degradation presents not as a sudden catastrophic failure, but as a slow, progressive decline in stability. The most frequent symptom reported by surgical staff is vertical drift or horizontal wobbling during heavy manipulations. When a platform cannot maintain absolute rigidity, it introduces micro-vibrations that interfere with delicate procedures, particularly in neurosurgery or ophthalmology.
The root cause of this instability often stems from a fundamental misunderstanding of static versus dynamic load ratings. Procurement teams frequently review the maximum static load capacity—the amount of weight the platform can hold while completely stationary. However, clinical reality involves dynamic loading. When a large patient is being shifted, or when a surgeon leans against the edge of the V-top panels, the torque applied to the lifting column multiplies significantly. If the internal lift mechanism was specified only for static resistance, the internal seals of a fluid-based cylinder will prematurely degrade, or the gears in an electric motor will strip.
Another major contributor to underperformance is structural torsion. Platforms constructed with inferior stainless steel grades, such as 201 series, lack the tensile strength of 304-grade steel. Over time, the continuous exposure to corrosive disinfectants and bodily fluids weakens the structural integrity of the joints, leading to a tabletop that flexes under pressure. This flexing exacerbates the strain on the central lifting column, creating a cycle of accelerating wear and tear.

Root Cause Analysis: Spec Mismatch in Lift Mechanisms
The debate between electric and fluid-driven lift systems often misses the core issue: environmental and workflow application. Both technologies are robust when properly matched to their intended clinical scenario, but misapplication guarantees a low return on investment.
Fluid-driven lift mechanisms rely on a sealed cylinder and a manual or powered pump. They are inherently durable and capable of lifting substantial weight. The primary failure mode here is seal degradation. In an emergency room setting where the platform is rapidly pumped up and down dozens of times a shift, the friction generates heat, which degrades the internal O-rings. Once a seal is compromised, microscopic amounts of fluid bypass the valve, resulting in the dreaded slow drift during surgery. The root cause is specifying a standard-duty pump for a heavy-duty, high-throughput environment.
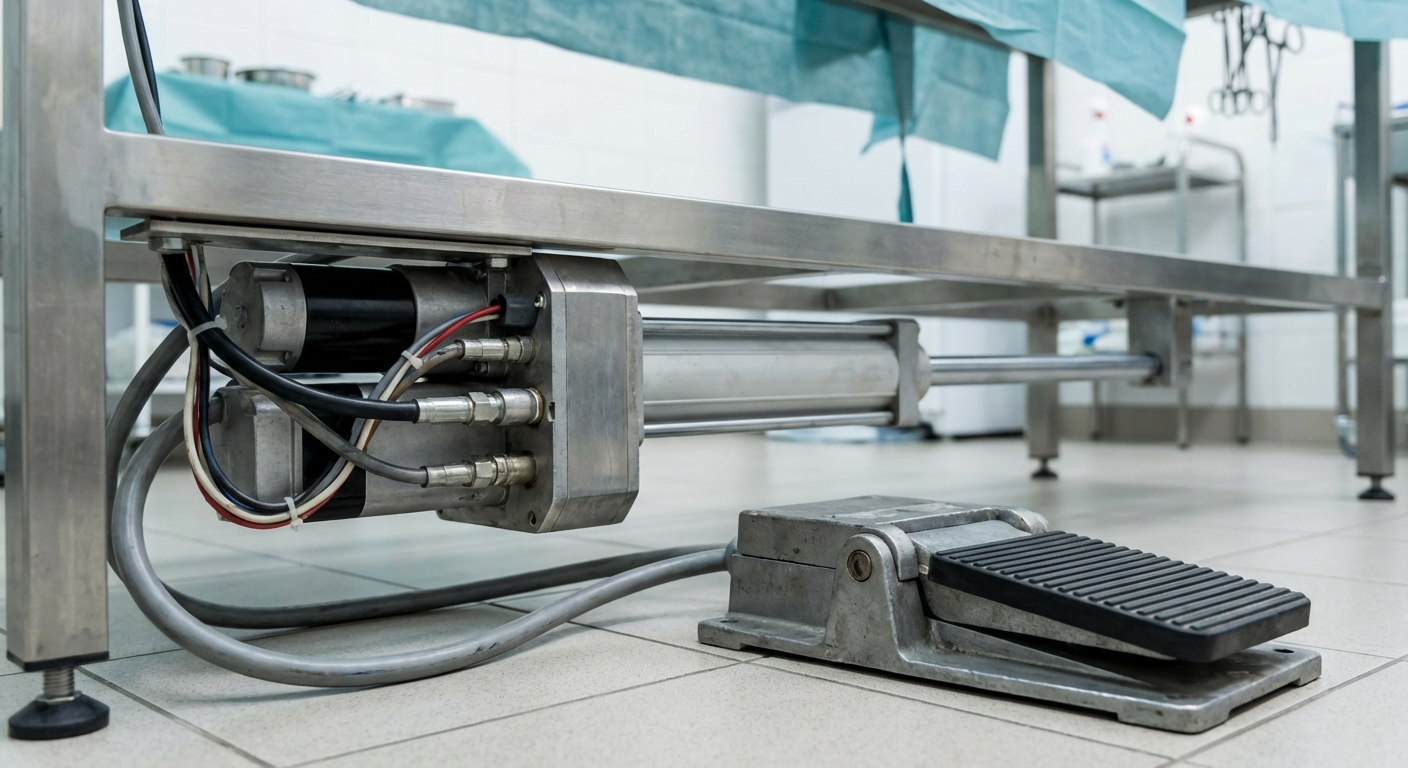
Conversely, motor-driven electric actuators offer exceptionally smooth, foot-pedal-operated height adjustments, allowing the surgeon to maintain sterility while repositioning the patient. However, electric systems are highly sensitive to side-loading. If an electric column designed for a 150kg straight vertical lift is repeatedly subjected to off-center weight distribution—such as a large canine resting entirely on one side of an extended V-top—the lateral stress will bend the internal drive screw or overheat the motor. Furthermore, electric systems in wet environments must possess an adequate Ingress Protection (IP) rating. Using a motor with a low IP rating in a suite where aggressive chemical washdowns are standard will inevitably lead to circuit shorts and actuator failure.
When evaluating options, facility managers often look for competitive mid-range pricing combined with factory-direct cost advantages. The HQS Medical product line is engineered precisely for this market gap. By integrating high-torque, IP66-rated electric actuators with 304-grade stainless steel V-top panels, these models provide a core advantage in high-volume orthopedic and soft-tissue surgical suites. Based on HQS clinical observation, clinics upgrading to these properly specified units see a significant reduction in patient repositioning time and a near-total elimination of mid-surgery vertical drift, making them highly applicable for both standard small animal practices and heavy-duty emergency centers.
Safety Thresholds & Evidence-Based Parameters
To ensure clinical safety and equipment longevity, procurement protocols must mandate strict adherence to established mechanical thresholds. Evaluating equipment without demanding verifiable parameters leaves the facility vulnerable to structural failures.
According to general principles derived from medical device safety standards for operating tables, a professional-grade unit must demonstrate a dynamic load threshold that exceeds the heaviest expected patient by at least a factor of 1.5. For a mixed-animal practice treating large canine breeds, the dynamic load capacity should be explicitly rated at 150 kg or higher, while the static hold capacity must exceed 250 kg. Platforms intended for exotic heavy stock or equine foal procedures demand static capacities exceeding 300 kg.
Furthermore, tilt mechanisms—essential for Trendelenburg or anti-Trendelenburg positioning to manage patient hemodynamics—must lock securely at specific angles. Evidence-based clinical guidelines require a minimum tilt range of +15° to -15°. The locking mechanism, whether manual or motor-driven, must demonstrate zero degree slippage when a 100 kg offset load is applied to the extreme end of the platform. Actuator noise is another critical parameter; motors should operate below 50 decibels (dB) to prevent startling recovering patients or disrupting communication among the surgical team.
Methodology & Verification Protocol
Claims of durability and weight limits must be subjected to rigorous empirical verification. A robust methodology for assessing table performance involves isolating the variables of vertical lift, lateral stability, and material endurance under simulated clinical extremes.
Verification protocols begin with load distribution testing. This is executed by placing precisely calibrated cast iron weights, totaling 150 kg, asymmetrically on the platform. A laser micrometer, operating with a 500Hz sampling rate, measures the vertical deflection of the tabletop edges. A compliant unit will show less than 2 millimeters of deflection under maximum asymmetric load.
Actuator lifecycle testing is equally critical. For electric units, the protocol demands running the lift mechanism through 10,000 continuous full-stroke cycles with a 100 kg load, while thermal imaging monitors the motor housing to ensure operating temperatures do not exceed the manufacturer's safety threshold. For fluid-based systems, pressure gauges are installed in-line to monitor internal cylinder pressure over a 48-hour static hold test. A pressure drop exceeding 2% indicates microscopic seal leakage, resulting in an immediate failure of the verification protocol.
Problem → Cause → Fix Matrix
Diagnosing operational issues rapidly is essential for minimizing facility downtime. The following matrix outlines the most frequent mechanical failures, their underlying engineering causes, and the appropriate corrective actions.
Symptom / Problem | Root Cause Analysis | Corrective Action / Fix |
|---|---|---|
Slow vertical drift during heavy surgical procedures. | Microscopic wear on hydraulic cylinder O-rings or bypass valve fluid leak due to exceeding dynamic load limits. | Rebuild the cylinder with high-density polyurethane seals and recalibrate the bypass valve. If recurring, upgrade to a higher-capacity electric actuator. |
Electric lift motor stalls or emits a burning odor mid-adjustment. | Lateral binding of the internal drive screw due to asymmetric patient weight distribution or motor thermal overload. | Implement a mandatory cool-down period. Inspect the lifting column for lateral bending. Replace the actuator with an IP66-rated, high-torque model. |
Surface rust and pitting on the V-top panels or drainage troughs. | Utilization of inferior 201-grade stainless steel combined with prolonged exposure to iodine or chloride-based disinfectants. | Institute a strict post-op fresh-water rinse protocol. For future procurement, mandate strictly 304 or 316-grade stainless steel construction. |
Wobbling or instability when locking mechanisms are engaged. | Worn mechanical linkages in the tilt gears or degradation of the floor-locking casters due to chemical floor cleaners. | Replace casters with chemical-resistant polyurethane wheels and re-torque all chassis linkage bolts to factory tension specifications. |
5 Red Flags in Supplier Proposals
Procurement teams must critically assess supplier proposals to identify hidden vulnerabilities that could inflate the Total Cost of Ownership (TCO). Identifying these red flags early prevents long-term maintenance disasters.
First, vague or absent IP (Ingress Protection) ratings for electronic components. Operating rooms are wet environments. If a proposal for an electric unit does not explicitly state an IP54 or higher rating for the control box and IP66 for the actuators, the equipment is highly susceptible to liquid damage from routine washdowns or biological fluid spills.
Second, a lack of distinction between static and dynamic load capacities. A proposal boasting a "300 kg weight limit" without specifying whether this applies to an actively moving platform or a stationary one is deliberately masking operational limitations. Always demand the dynamic lifting capacity.
Third, ambiguous material specifications. Phrases like "high-quality stainless steel" are meaningless. Suppliers must provide the exact metallurgical grade, preferably 304 or 316 stainless steel. Lower grades will corrode rapidly in a clinical environment, leading to contamination risks.
Fourth, proprietary electronic architectures that lock facilities out of third-party repairs. If the control board requires specialized, brand-locked diagnostic software to replace a simple foot pedal, the hospital will face exorbitant service fees and prolonged downtime. Open-architecture electronic components are vital for continuous operation.
Fifth, fragmented warranty terms. A common tactic is offering a "5-year warranty" that applies only to the steel frame, while burying a 90-day limit on fluid seals, electric motors, and control pedals in the fine print. Comprehensive coverage must extend to the high-wear kinetic components.

Avoiding Repeat Procurement Failures
Establishing a rigorous, standardized selection process is the only way to break the cycle of reactive purchasing and equipment failure. Procurement professionals must align the mechanical specifications directly with the facility's most demanding clinical workflows. For instance, while a basic flat-top unit may suffice for a low-volume vaccination clinic, an emergency center performing complex abdominal surgeries requires independent V-top adjustability and powered tilt functions.
Integration with existing infrastructure is also paramount. The dimensions of the chassis must accommodate the ergonomic positioning of the surgical team and the placement of auxiliary equipment, such as a high-definition veterinary patient monitor and overhead lighting systems. A holistic procurement approach evaluates how the central operating platform interacts with the entire spatial footprint of the suite.
Equipment Type | Key Specifications & Lift Mechanism | Optimal Clinical Scenarios | Relative Price & ROI Profile |
|---|---|---|---|
Electric V-Top System | IP66 dual actuators, independent lateral tilt, 150kg+ dynamic load. | High-volume orthopedics, complex abdominal surgeries, neurology. | Premium initial cost; excellent long-term ROI due to ergonomic efficiency. |
Hydraulic Flat Top | Closed-loop fluid pump, single-column lift, 200kg static capacity. | General practice, basic spay/neuter clinics, outpatient minor procedures. | Lower initial cost; moderate ROI depending on frequency of seal maintenance. |
Electric-Hydraulic Hybrid | Motor-driven fluid pump, superior vibration dampening. | Heavy animal practices, exotic stock, sensitive microsurgery. | Highest initial cost; excellent ROI for specialized heavy-load facilities. |
Manual Scissor Lift | Mechanical gear or basic gas strut, manual elevation locking. | Field operations, mobile clinics, secondary prep rooms. | Lowest initial cost; fast ROI but limited clinical application scope. |
Frequently Asked Questions
How do we calculate the required dynamic load capacity for a mixed-animal practice?
To calculate the required dynamic load capacity, identify the 95th percentile weight of your heaviest patient demographic and multiply by a safety factor of 1.5. For a practice treating large breeds weighing up to 80 kg, the lift mechanism must comfortably support continuous, smooth movement of at least 120 kg to prevent motor burnout or seal failure.
What is the average lifespan of an electric lift actuator versus a fluid-driven pump?
Under rigorous clinical conditions, a high-quality, IP66-rated electric actuator typically operates reliably for 7 to 10 years before requiring component replacement, provided it is not subjected to severe side-loading. Fluid-driven pumps generally require minor maintenance, such as seal replacements, every 3 to 5 years, but the core cylinder can last over 15 years with proper fluid management.
Can internal fluid leaks in lift columns be prevented through routine maintenance?
Yes. The vast majority of fluid leaks are caused by particulate contamination entering the cylinder through worn wiper seals or by operating the pump when the internal fluid level is critically low. Establishing a bi-annual maintenance protocol to clean the external piston rod, inspect wiper seals, and verify fluid viscosity will prevent 90% of premature leakage failures.
Does the steel grade significantly impact the longevity of the surgical surface?
Absolutely. Type 304 stainless steel contains chromium and nickel, providing robust resistance to oxidation and harsh chemical disinfectants used in clinical settings. Lower grades, like 201, lack sufficient nickel content and will quickly develop micropitting and rust spots when repeatedly exposed to biological fluids and chloride-based cleaners, compromising sterility.
Clinical Implementation Roadmap
Procuring the optimal operating platform is only the first phase; maintaining its performance requires a strategic implementation and maintenance roadmap. Establish a clear protocol for the surgical team regarding weight distribution. Staff must be trained to center heavy patients over the lifting column rather than at the extreme edges, drastically reducing off-center torque on the actuators.
Next, implement a preventative maintenance schedule that moves beyond simple surface cleaning. For electric systems, this involves quarterly inspections of the wiring harnesses, foot pedal contacts, and a functional test of the limit switches. For fluid-driven models, technicians must verify the integrity of the release valves and check for micro-leaks around the base of the cylinder during maximum load tests.
Finally, integrate the equipment into your digital asset management system. Track the frequency of use, documented maintenance interventions, and any staff reports of minor instability or abnormal noise. By shifting from a reactive repair model to a proactive surveillance protocol, clinical directors can extend the operational life of their infrastructure, ensure uninterrupted workflow, and maximize the financial return on their capital investments.