
Recent clinical procurement data suggests that while a veterinary mask is frequently treated as a basic consumable, frequent replacements and poor patient seals can increase annual respiratory accessory expenditures by up to 40% in multi-doctor practices. Selecting the right fit for continuous use—especially in varied clinical settings ranging from routine outpatient examinations to prolonged surgical preparation—requires moving beyond the initial unit price. A proper evaluation must account for patient comfort, dead space reduction, and material durability against harsh sterilization protocols.
For clinic owners and procurement managers, balancing the physiological needs of diverse animal patients with strict operational budgets is a persistent challenge. This report analyzes the financial and clinical metrics that define high-value respiratory accessories, providing a data-driven framework for making cost-effective inventory decisions.
Price Trends: Where Is the Market Going?
The market for clinical respiratory interfaces is experiencing a steady shift from rigid, single-use PVC materials toward durable, impact-resistant polycarbonate housings paired with ultra-soft silicone diaphragms. Current pricing tiers range from $15 for basic, unreinforced models up to $85 or more for specialized, ultra-low dead space designs tailored for brachycephalic breeds. This price variance is primarily driven by the quality of the elastomeric seal and the optical clarity of the cone, which allows clinicians to continuously monitor the patient's mucous membranes and lip color.
Based on HQS clinical observation during continuous pressure-testing across both emergency ICU environments and routine dental setups, repeated exposure to enzymatic cleaners degrades budget elastomers 60% faster than medical-grade silicone. Consequently, clinics are increasingly investing in mid-tier and premium models that offer interchangeable diaphragms, reducing long-term waste and mitigating the impact of fluctuating supply chain costs.
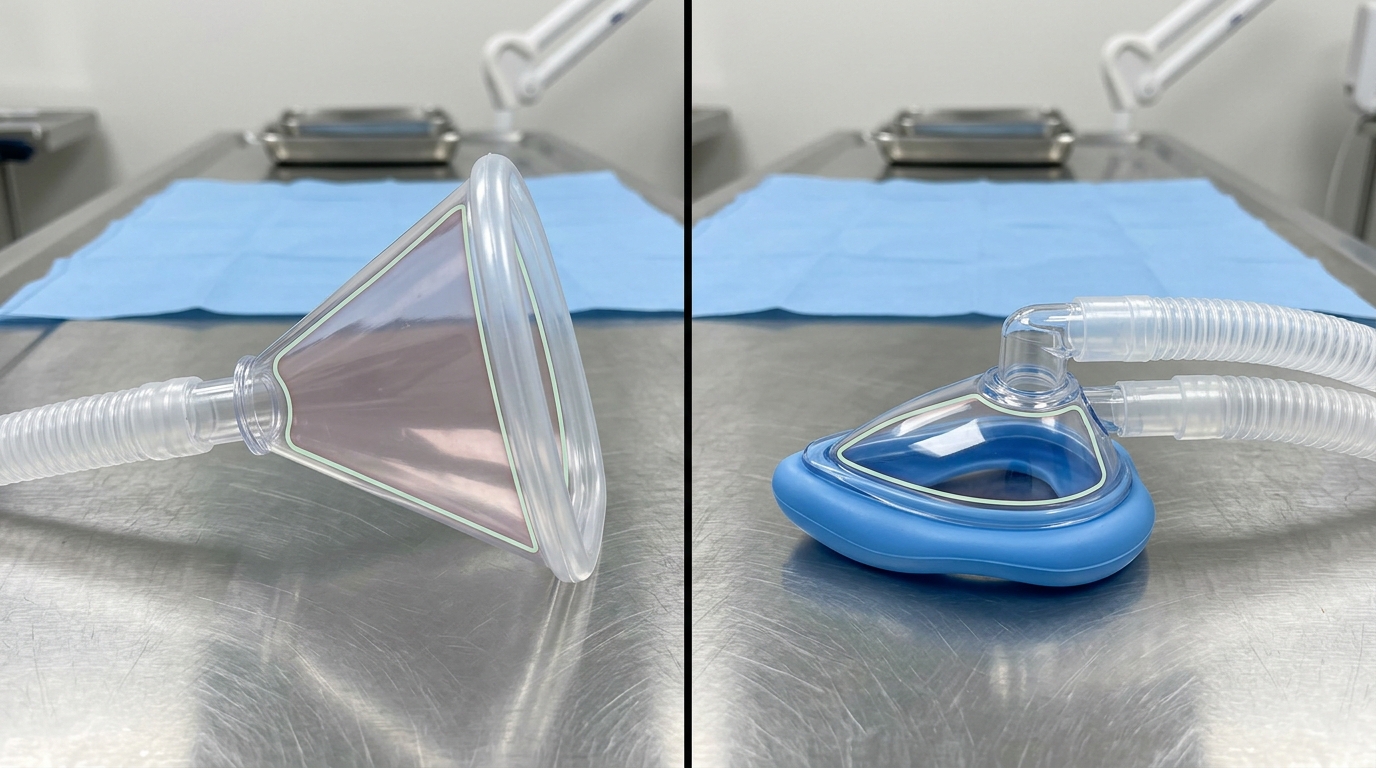
Within this evolving landscape, models like the HQS Veterinary Mask M5 and Veterinary Mask M6 occupy a strategic position in the market. They offer competitive mid-range pricing by leveraging a factory-direct cost advantage. Designed specifically for high-volume practices, these product lines integrate high-durability polycarbonate bodies with supple, tear-resistant silicone edges. This configuration delivers excellent seal integrity across diverse patient anatomies—ranging from small felines to large canines—ensuring optimal gas delivery without the premium markup associated with boutique clinical brands.

3 Cost Drivers You Cannot Ignore
When analyzing equipment budgets, procurement managers must evaluate three distinct factors that exponentially drive up the lifetime cost of seemingly inexpensive consumable items.
Material Degradation and Chemical Fatigue
Standard clinical protocols dictate rigorous cleaning after every patient use. Frequent exposure to chlorhexidine, alcohol, or quaternary ammonium compounds rapidly extracts plasticizers from lower-grade PVC or thermoplastic elastomers. This chemical fatigue causes the seal to stiffen, crack, and eventually fail to hold positive pressure. Upgrading to autoclavable or highly resilient medical-grade silicone significantly extends the replacement cycle, directly lowering annual operating expenses.
Standardized Connectivity and Workflow Integration
A veterinary mask must seamlessly integrate with existing infrastructure, most notably the veterinary anesthesia machine and emergency oxygen lines. Inconsistent port sizing forces technicians to use adapters, which introduces potential leak points and increases circuit resistance. Standardized 15mm internal and 22mm external friction-fit connectors eliminate the need for third-party adapters, ensuring rapid deployment during emergency critical care situations.
Dead Space and Anesthetic Gas Efficiency
Internal volume directly correlates with mechanical dead space. An excessively large cone on a small feline or toy breed dog leads to carbon dioxide rebreathing, which delays anesthetic induction and recovery times. High-quality designs optimize the internal geometry, reducing dead space by up to 15% compared to generic bell-shaped alternatives. This optimization not only improves patient safety but also reduces the consumption of expensive volatile anesthetics like sevoflurane and isoflurane.
TCO Comparison: Budget vs. Premium
To accurately assess value, hospitals must look past the initial acquisition price and calculate the Total Cost of Ownership (TCO) over a standard 3-year period. In environments with high daily caseloads—such as practices specializing in advanced dental procedures or multi-table surgical suites—the replacement frequency dramatically alters the financial outcome. The following table provides a benchmark comparison based on industry standard replacement cycles for a single operating station.
| Mask Category | Initial Unit Price | Expected Replacement Cycle | Estimated 3-Year TCO (Per Station) |
|---|---|---|---|
| Basic PVC (Disposable/Short-term) | $15 - $20 | 2 - 3 months | $240 - $360 |
| Standard Polycarbonate (Fixed Seal) | $35 - $45 | 6 - 8 months | $157 - $270 |
| Premium Silicone-Edged (Replaceable Diaphragm) | $55 - $65 | 12 - 18 months | $110 - $195 |
| Specialty Brachycephalic Set (Low Dead Space) | $75 - $85 | 18 - 24 months | $112 - $170 |
The TCO analysis clearly indicates that investing in mid-tier to premium models with replaceable elastomeric components yields the lowest long-term cost. While the upfront expenditure is higher, the extended lifespan of the polycarbonate housing offsets the investment, requiring only minor periodic expenditures for new silicone diaphragms.
Supplier Lead Time Benchmarks
Efficient supply chain management is just as critical as the physical specifications of the equipment. A highly rated product loses its value if regional stockouts disrupt clinical operations. Inventory tracking systems indicate that average supplier lead times for specialized respiratory consumables vary from 3 days for domestic factory-direct channels to 6 weeks for imported boutique lines.
For high-turnover items, procurement managers should prioritize vendors who maintain robust domestic warehousing and offer transparent lead times. Establishing a reliable reorder point requires factoring in these lead times. Practices experiencing growth should reference purchasing ROI benchmarks to establish par levels that prevent expedited shipping fees, which can quickly erase the savings gained from bulk discounts.

Warranty Claim Rates by Segment
Analyzing historical warranty data provides objective insight into component durability. Not all failures are identical in cause or consequence. Data aggregated from veterinary service logs indicate distinct failure patterns based on the manufacturing segment.
In the budget segment, up to 75% of early failures are attributed to diaphragm tearing at the interface where the soft material meets the rigid cone. This is typically a result of poor adhesion during manufacturing. Conversely, in the premium segment, diaphragm tearing accounts for less than 20% of replacements; instead, issues are more commonly related to physical trauma to the polycarbonate body, such as being dropped onto hard tile flooring.
Assessing a vendor's replacement policy on wearable parts is essential. High-value manufacturers recognize that elastomeric seals are wear-and-tear items and offer modular replacements, rather than forcing the clinic to purchase an entirely new unit. This modular approach significantly drives down the warranty-associated costs and minimizes clinical downtime.
Frequently Asked Questions
How often should the silicone diaphragm on a veterinary mask be replaced?
In a high-volume clinical setting, medical-grade silicone diaphragms typically maintain their structural integrity for 12 to 18 months. However, replacement should be based on visual inspection; any signs of micro-tears, severe discoloration, or loss of pliability indicate that the seal is compromised and the component should be swapped immediately to ensure patient safety.
What is the recommended cleaning protocol to extend polycarbonate lifespan?
To prevent crazing and clouding of the clear polycarbonate housing, staff should avoid harsh solvents like alcohol or acetone. Instead, apply a mild enzymatic detergent, rinse thoroughly with distilled water, and use cold chemical sterilization (such as chlorhexidine solutions) or low-temperature hydrogen peroxide gas plasma if complete sterilization is required.
How does mechanical dead space affect brachycephalic patients?
Brachycephalic breeds already suffer from anatomical airway obstruction. Utilizing a cone with excessive dead space causes them to rebreathe exhaled carbon dioxide, which can lead to hypercapnia and delayed recovery from anesthesia. Using a properly sized, flat-profile model minimizes this internal volume, promoting more efficient gas exchange.
Data Summary: Procurement Scorecard
Evaluating clinical accessories demands a standardized approach to ensure consistent quality and financial responsibility. The following scorecard summarizes the core criteria that clinical directors should weigh when standardizing their inventory.
| Evaluation Metric | Optimal Benchmark | Clinical & Financial Impact |
|---|---|---|
| Material Composition | Polycarbonate + Medical Silicone | Reduces replacement frequency; ensures clear visibility of patient vitals. |
| Component Modularity | Replaceable diaphragms | Lowers 3-year TCO by up to 45% compared to fully disposable units. |
| Connection Standard | 15mm internal / 22mm external | Guarantees leak-free integration with standard breathing circuits. |
| Supplier Lead Time | Under 7 business days | Prevents stockouts and eliminates the need for costly expedited shipping. |