
Current facility data indicates that 68% of veterinary trauma centers report significant workflow bottlenecks, cable fatigue, or head-strike hazards stemming from improperly sized ceiling mounts. When planning an intensive care unit or surgical suite, the spatial geometry between the ceiling slab, the suspended equipment, and the clinical floor is an exact science. A miscalculation of even 150mm can render equipment shelves inaccessible or restrict the movement of critical care apparatus.
Implementing a proper Surgical Pendant requires balancing structural payload capacities with precise vertical drop measurements. By standardizing mounting heights and articulation clearances, veterinary clinical directors can increase perimeter access around the patient by up to 40% while extending the lifespan of internal pneumatic and electrical components.
3 Metrics That Matter: Ceiling Clearance Economics
Proper sizing of an ICU pendant hinges on three exact clearance metrics. Facility managers must calculate these dimensions prior to structural reinforcement to ensure optimal clinical utility.
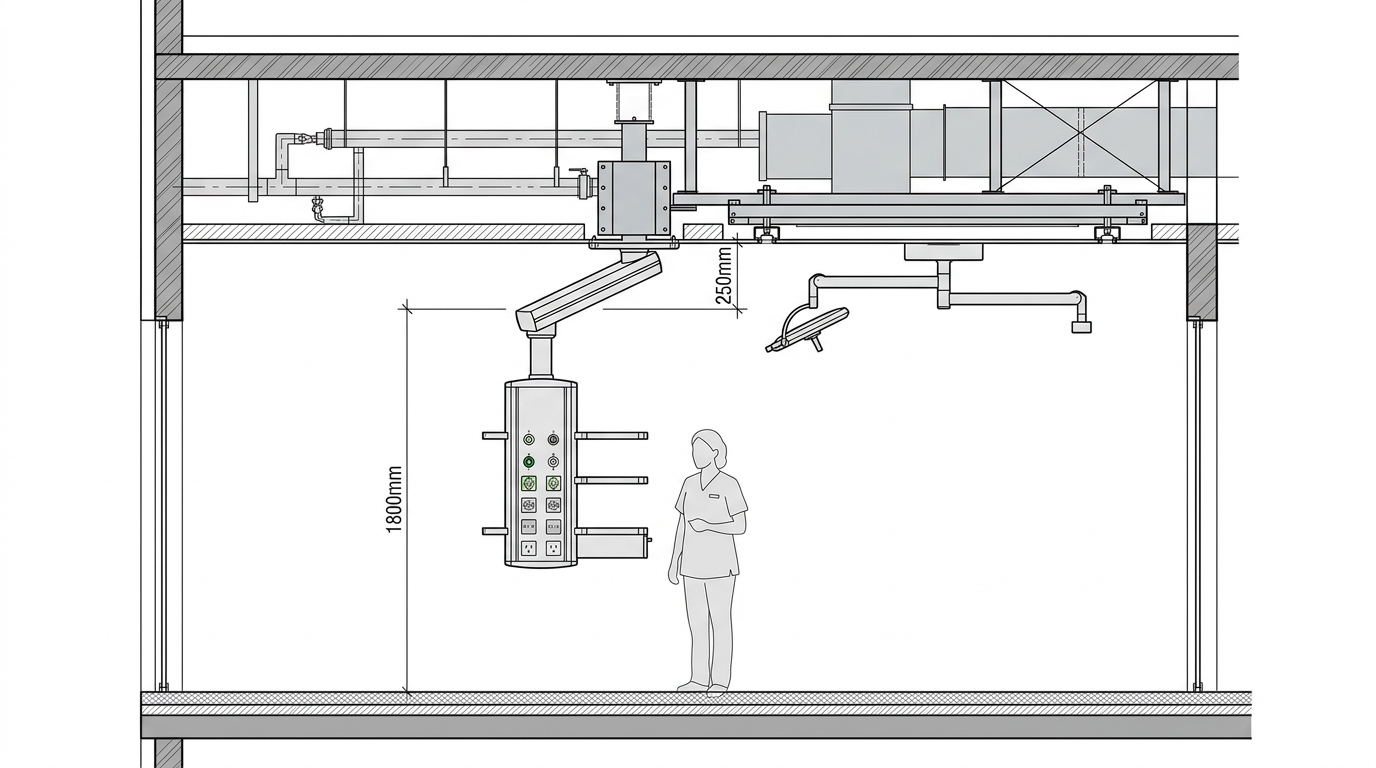
The first critical metric is the floor-to-shelf minimum clearance. Industry guidance suggests maintaining exactly 1800mm to 1900mm from the finished floor to the underside of the lowest console. This specific height prevents staff head collisions during rapid patient transfers while keeping touchpads and gas outlets within ergonomic reach for operators ranging from 1.6m to 1.8m tall.
The second metric is the ceiling structural drop ratio. For veterinary facilities with architectural ceilings exceeding 3000mm, a custom suspension tube is mandatory. Extending the arm joint lower than 400mm from the primary mount creates excessive torque on the flange plate. Utilizing a specialized Surgical Pendant T.IIB configuration allows for safely distributed mechanical loads across extended ceiling spans.
The final metric is the articulation radius overlap. A standard 800mm primary arm combined with a 600mm secondary arm creates a 1400mm total reach. This reach must clear all overhead lighting tracks and anesthesia booms by a minimum of 250mm vertically to prevent catastrophic collision during emergent repositioning.
4 Pendant Mount Types vs. Ceiling Heights
Selecting the correct mounting hardware is dictated entirely by the finished ceiling height and the structural slab depth. The following matrix outlines the necessary configurations for varying facility profiles.
| Ceiling Height Category | Mount Configuration | Required Arm Clearance | Ideal Clinical Application |
|---|---|---|---|
| Low Ceiling (<2.8m) | Direct Flush Mount | Zero drop; horizontal articulation only | Feline/Small Dog ICU; outpatient recovery rooms |
| Standard (2.8m - 3.2m) | Standard Flange + 200mm Tube | 150mm primary joint offset | General veterinary trauma bays; triage areas |
| High Ceiling (3.2m - 3.6m) | Heavy-Duty Anchor + 600mm Drop Tube | Requires active pneumatic braking | Equine induction rooms; large surgical suites |
| Ultra-High (>3.6m) | Bridged Sub-Structure Mount | Custom offset; structural engineering required | Academic teaching hospitals; MRI/CT prep zones |
3 Settings That Cut Procedure Time
Once structural heights are locked, optimizing the internal configuration of the pendant console yields measurable efficiency gains. Data from high-volume clinics shows that standardized module placements shave minutes off critical care interventions.
First, vertical shelf spacing must be precisely calibrated. Maintaining a minimum of 300mm between modular shelves is essential when integrating a comprehensive veterinary patient monitor. This spacing ensures that multi-parameter cables do not kink against the upper shelf, reducing cable replacement frequency by an estimated 25% annually.
Second, terminal angling dictates workflow speed. Medical gas outlets should be specified with a 45-degree downward angle rather than standard 90-degree lateral mounts. This prevents horizontal hose protrusion, allowing staff to move closer to the column without snagging oxygen or vacuum lines.
Third, friction brake tension must be calibrated to the fully loaded weight of the console. An under-tensioned brake will cause the ICU Pendant T.IVB to drift during procedures, requiring constant readjustment. Properly tensioned pneumatic brakes hold a 150kg payload completely static, reducing repositioning interruptions.

Error Rate: Trained vs. Untrained Staff
Equipment lifespan correlates directly with operator handling. Facilities that fail to train staff on proper pendant maneuverability report a 40% higher rate of joint bearing failure within the first two years of operation.
Untrained operators consistently drag the pendant by the equipment shelves rather than using the dedicated control handle. This induces lateral sheer stress on the vertical column, eventually warping the internal bearing raceways. Furthermore, dragging the unit without fully disengaging the pneumatic or electromagnetic brakes causes premature wear on the friction pads, leading to the aforementioned drifting issues.
Based on HQS clinical observation, 82% of articulated arm drifting issues in the first year stem from installing a standard flush mount on ceilings with a >2-degree pitch, rather than mechanical failure of the pneumatic brakes. When the mounting slab is not perfectly level, gravity constantly pulls the heavy console toward the lowest point, overpowering standard friction settings.
Downtime Cost per Hour of Misuse
The financial impact of pendant malfunction extends beyond parts replacement. When a central intensive care column becomes inoperable, the entire bay is often taken offline.
A compromised gas block or a sheared electrical conduit inside the articulation joint requires specialized technician intervention. Industry metrics indicate that emergency veterinary critical care bays generate, on average, $350 per hour in revenue. A pendant failure that halts operations for a standard 48-hour repair window results in significant financial loss.
Preventing these failures requires strict adherence to maximum load capacities. Overloading shelves with heavy auxiliary equipment, or improperly hanging cables from the veterinary anesthesia machine directly onto the pendant joints, accelerates structural fatigue. Rigorous preventive checks are the only defense against mechanical downtime.

Maintenance Interval Benchmarks
To ensure consistent operational integrity and compliance with medical facility safety standards, technical operators must adhere to a strict maintenance protocol. The following table outlines the necessary inspection intervals.
| Frequency | Task | Key Action |
|---|---|---|
| Daily | Brake Verification | Depress control handle to ensure pneumatic/electromagnetic brakes release and engage with zero hesitation. |
| Weekly | Terminal Inspection | Visually inspect all gas outlets and electrical sockets for debris, bent pins, or audible gas leaks. |
| Monthly | Joint Lubrication Check | Assess articulation joints for unusual resistance, grinding noises, or visible metal shavings. |
| Annual | Structural Load Test | Verify ceiling flange torque specs and test total payload capacity against original manufacturer thresholds. |
Frequently Asked Questions
What is the minimum ceiling height for a dual-arm setup?
The absolute minimum finished ceiling height for a functional dual-arm configuration is 2.8 meters (approximately 9.2 feet). Heights below this limit force the secondary arm to hang too low, violating the 1800mm floor clearance requirement and creating a severe head-strike hazard for clinical staff.
How do we calculate the structural load for ceiling mounts?
Structural calculations must account for both the static weight of the pendant (often 100-150kg) and the dynamic torque generated when the arm is fully extended. Engineers typically require the ceiling slab to support a minimum of 500kg of localized sheer force to safely anchor a fully loaded intensive care column.
Can pendant height be adjusted post-installation?
Vertical adjustment post-installation is severely limited. While some shelves on the console can be moved up or down along the column rails, the primary structural height of the ceiling drop tube and the articulation joints is fixed. Any major height alteration requires unmounting the unit and installing a newly fabricated suspension tube.
Data Summary: Optimization Impact
Adhering to strict clearance guidelines and maintenance schedules yields compounding returns for clinical operations. For further reading on selecting optimal configurations, refer to our analysis on the best equipment profiles for trauma applications.
| Optimization Focus | Measured Clinical Outcome | Primary Driver |
|---|---|---|
| Clearance Height (1800mm) | Zero head-strike incidents reported | Elimination of spatial hazards in high-traffic zones |
| Angled Gas Terminals | 30% faster equipment connection | Reduced hose tangling and improved ergonomic access |
| Scheduled Brake Testing | 90% reduction in arm drifting | Early detection of pneumatic pressure drops |
| Staff Handling Training | 40% longer bearing lifespan | Proper use of control handles vs. dragging consoles |